ebanga™ (ansuvimab-zykl)
FOR INJECTION / 400 mg per vial
EBANGA™
The only FDA-approved lyophilized treatment for Orthoebolavirus zairense administered as a single 1-hour IV infusion.*
EBANGA™ is a Orthoebolavirus zairense glycoprotein (EBOV GP)-directed human monoclonal antibody indicated for the treatment of infection caused by Orthoebolavirus zairense in adult and pediatric patients, including neonates born to a mother who is Real-Time Polimerase Chain Reaction (RT-PCR) positive for Orthoebolavirus zairense infection
Limitation of Use
• The efficacy of EBANGA has not been established for other species of the Orthoebolavirus and Orthomarburgvirus genera.
• Orthoebolavirus zairense can change over time, and factors such as emergence of resistance or changes in viral virulence could diminish the clinical benefit of antiviral drugs. Consider available information on drug susceptibility patterns for circulating Orthoebolavirus zairense strains when deciding whether to use EBANGA.
* Infusions may be slowed or stopped if necessary, to alleviate any side effects.
Only approved in the US.
Orthoebolavirus zairense
Ebola virus disease (EVD), is a rare but severe, highly contagious and often fatal illness with an average case fatality rate of approximately 50%. Case fatality rates have ranged from 25% to 90% in past outbreaks. Ebola virus disease (who.int)
The 10th outbreak of EVD to affect the Democratic Republic if Congo (DRC) was declared on August 1, 2018(1). By the time the outbreak was declared over by the DRC Ministry of Health nearly two years later, 3,300 confirmed cases resulted in a 67% case fatality rate (CFR)(2). It is currently recognized as the longest outbreak in DRC history and the second largest Ebola epidemic ever recorded(3).
Four investigational therapies for EVD were studied in the DRC during the 10th outbreak, despite persistent security challenges, including militia attacks on the Ebola Treatment Units (ETUs) in the trial. The willingness of study participants to share their data in the hope for a cure, and the remarkable efforts of our colleagues in the ETUs who preserved the resulting study data through fires, site closures and municipal lockdowns are the champions who embody the study.
(1) Ebola | Ebola situatin reports: Democratic Republic of the Congo (Archive) (who.int)
(2) Ebola Virus Disease Outbreak - Democratic Republic of the Congo, August 2018-November 2019 (cdc.gov)
(3) DRC tenth Ebola outbreak (msf.org)
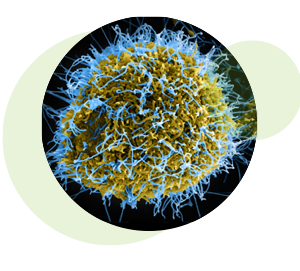 Colorized scanning electron micrograph of filamentous Ebola virus particles (blue) budding from a chronically infected VERO E6 cell (yellow-green). Credit: National Institute of Allergy and Infectious Diseases, NIH
Colorized scanning electron micrograph of filamentous Ebola virus particles (blue) budding from a chronically infected VERO E6 cell (yellow-green). Credit: National Institute of Allergy and Infectious Diseases, NIH
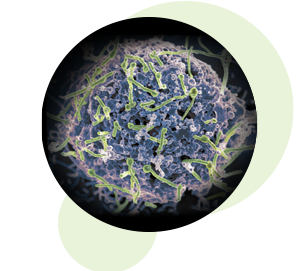 Ebola virus (green) is shown on cell surface.
Credit: National Institute of Allergy and Infectious Diseases, NIH
Ebola virus (green) is shown on cell surface.
Credit: National Institute of Allergy and Infectious Diseases, NIH
How it Works
EBANGA™ (ansuvimab-zykl, formerly known as mAb114) is a Orthoebolavirus zairense (EBOV) glycoprotein 1 (GP1)-directed recombinant, human Immunoglobulin G1 (IgG1) monoclonal antibody.
EBANGA™ is a single monoclonal antibody that was isolated from a human survivor of the 1995 Ebola outbreak in Kikwit, in the DRC. This human survivor maintained circulating antibodies against the Ebola virus surface glycoprotein for more than a decade after infection. (1)
The antibody was developed by scientists at the National Institute of Allergy and Infectious Diseases (NIAID), who discovered these Ebola virus antibodies in the blood samples from that survivor. Investigators from the Institute for Research in Biomedicine in Switzerland isolated the specific antibodies to test for potential efficacy in treating Ebola virus infection. (2)
NIAID and Dartmouth College researchers then studied how Ebanga™ (ansuvimab-zykl) neutralizes the Ebola virus and determined that it binds to the core of the Ebola glycoprotein, blocking its interaction with a receptor on human cells. This area of the Ebola glycoprotein, called the receptor binding domain, was previously thought to be unreachable by antibodies because it is well-hidden by other parts of the virus, and only becomes exposed after the virus enters the inside of cells. (2)
From that survivor of the 1995 Kikwit outbreak, monoclonal antibodies (mAbs) were isolated that neutralize recent and previous outbreak variants of the Ebola virus and mediate antibody-dependent cell-mediated cytotoxicity in vitro. (1)
(1) Protective monotherapy against lethal Ebola virus infection by a potently neutralizing antibody - PubMed (nih.gov)
(2) Antibody From Human Survivor Protects Macaques Against Ebola | Global Biodefense
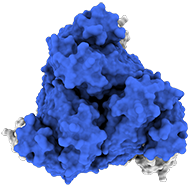
Top view:
Model of the antigen-binding fragment of the monoclonal antibody EBANGA&tm; (blue) in complex with the mucin-like domain deleted form of the Ebola virus GP (grey)
Credit: J. Misasi et al, NIAID
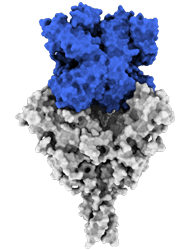
Side view:
Model of the antigen-binding fragment of the monoclonal antibody EBANGA™ (blue) in complex with the mucin-like domain deleted form of the Ebola virus GP (grey)
Credit: J. Misasi et al, NIAID
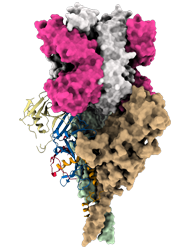
Model of mucin-like domain deleted form of the Ebola Glycoprotein (GP∆Muc) in complex with the antigen-binding fragment (Fab) of the monoclonal antibody EBANGA TM . EBANGA TM Fabs (heavy chain in pink and light chain in white) bind in a near-vertical orientation to the central chalice of GP∆Muc trimer, primarily making contact with the core region GP1. Two of three Fabs are visualized in this side view. Molecular surfaces of two GP∆ Muc protomers are colored in green and beige, whereas the third protomer is shown as a ribbon representation with colors representing various regions of Ebola GP.
Credit: J. Misasi et al, NIAID
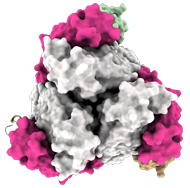
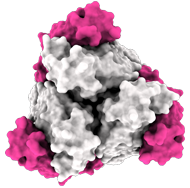
In top view (900 rotation):
3 Fab EBANGA™ bind to Ebola GP∆Muc trimer.
Credit: J. Misasi et al, NIAID
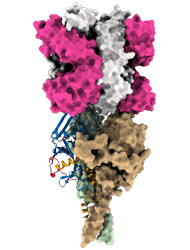
Model of the predicted Ebola Glycoprotein following cathepsin cleavage (GPcl) in complex with the antigen-binding fragment (Fab) of the monoclonal antibody EBANGA TM . EBANGA TM makes contact with the only surface exposed residues of the receptor binding domain (RBD) in the uncleaved GP and obstructs access to the remaining RBD residue that are exposed following cathepsin cleavage. In this manner, EBANGA TM prevents the Ebola GP from binding to its receptor protein, NPC1, and blocks infection. Molecular surfaces of two GP∆Muc protomers are colored in green and beige, whereas the third protomer is shown as a ribbon representation with colors representing various regions of
Credit: J. Misasi et al, NIAID
Side view:
Model of the antigen-binding fragment of the monoclonal antibody EBANGA™ (blue) in complex with the mucin-like domain deleted form of the Ebola virus GP (grey)
Credit: J. Misasi et al, NIAID
PAmoja TuLinde Maisha (PALM) Trial
The 10th outbreak of EVD to affect the DRC was declared on 1 August 2018. (1) By the time the outbreak was declared over by the DRC Ministry of Health nearly two years later, 3,300 confirmed cases resulted in a 67% case fatality rate (CFR). (2) It is currently recognized as the longest outbreak in DRC history and the second largest Ebola epidemic ever recorded. (3)
In November 2018, the National Institutes of Health (NIH), National Institute of Allergy and Infectious Diseases (NIAID) and the Institut National de Recherche Biomédicale (INRB) of the Democratic Republic of Congo (DRC) began a Phase 2/3 clinical trial testing multiple investigational Ebola therapies. The PALM trial was conducted by a research consortium overseen by the World Health Organization (WHO) that included nongovernment organizations and the DRC Ministry of Health. (1)
The PALM trial was a multicenter, open-label, randomized, controlled trial initiated in 2018 in the DRC to evaluate the safety and efficacy of four investigational therapies for EVD. The PALM trial was jointly sponsored by the WHO, the NIH and the INRB in the DRC.
The study was designed to compare mortality among patients receiving one of three investigational drugs (EBANGA™ [formerly mAb114], REGN-EB3 and remdesivir) with a control group of patients receiving the investigational monoclonal antibody cocktail treatment, ZMapp. (2)
Preliminary results announced in August 2019 prompted an independent data and safety monitoring board (DSMB) to recommend the study be stopped and that all future patients be randomized to receive either EBANGA™ or REGN-EB3 in an extension phase of the study. (1)
(1) Ebola | Ebola situation reports: Democratic Republic of the Congo (Archive) (who.int)
(2) Ebola Virus Disease Outbreak — Democratic Republic of the Congo, August 2018–November 2019 (cdc.gov)
(3) DRC tenth Ebola outbreak (msf.org)
In the PALM trial, 174 subjects (120 adults and 54 pediatric subjects) with confirmed Zaire ebolavirus infection were treated with EBANGA™ and 168 subjects were treated with the investigational control. All subjects received optimized standard of care treatment (oSOC). The primary efficacy endpoint was 28-day mortality.
35% of EBANGA™-treated subjects died by Day 28, compared to 49% in the control group (-14.3% difference, 95% confidence interval [CI]: -24.7, -3.7, p=0.008)
Among subjects with a low viral load (CtNP > 22)(1) at baseline, 10% of EBANGA™-treated subjects died by Day 28, compared to 24% in the control group (-13.8% difference, 95% CI: -27.3, 0.3)
(1) CtNP refers to “cycle threshold for the nucleoprotein gene”, a measure to determine viral load in the bloodstream
| ADVERSE EVENT a | EBANGA™ (N=173) % |
Control b (N=168) % |
|---|---|---|
| Pyrexia | 17 | 58 |
| Tachycardia | 9 | 32 |
| Diarrhea c | 9 | 18 |
| Vomiting c | 8 | 23 |
| Hypotension | 8 | 31 |
| Tachypnea | 6 | 28 |
| Chills d | 5 | 33 |
| Hypoxia c | 3 | 11 |
a Adverse events in this table were reported on the day of infusion, and included signs and symptoms that occurred during or immediately after infusion
b Investigational therapy administered as three separate infusions
c Adverse events that occurred during infusion but were not pre-specified.
d The term chills includes other similar adverse events including rigors and tremors
Each dose was delivered via intravenous (IV) infusion by a healthcare professional. Hypersensitivity reactions including infusion-associated events have been reported during and post-infusion with EBANGA™. Approximately 99% of subjects who received EBANGA™ in the PALM trial were able to complete their dose within one hour. Two subjects who received EBANGA™ (1%) did not receive their complete infusion. In eight subjects (5%) the EBANGA™ infusion rate was decreased due to an adverse event. The adverse event profile in adult and pediatric subjects treated with EBANGA™ was similar. The evaluation of adverse events in subjects who received EBANGA™ may have been confounded by signs and symptoms of the underlying Orthoebolavirus zairense infection.
| LABORATORY TEST a | EBANGA™ (N=173) % |
Control (N=168) % |
|---|---|---|
| Sodium, high ≥ 154 mmol/L | 5 | 4 |
| Sodium, low < 125 mmol/L | 7 | 11 |
| Potassium, high ≥ 6.5 mmol/L | 15 | 12 |
| Potassium, low < 2.5 mmol/L | 6 | 8 |
| Creatinine (mg/dL) > 1.8 x ULN or ≥ 1.5 x baseline b | 27 | 23 |
| Alanine aminotransferase (U/L) ≥ 5 x ULN c | 12 | 14 |
| Aspartate aminotransferase (U/L) ≥ 5 x ULN d | 13 | 18 |
ULN = upper limit of normal
a Graded per Division of AIDS (DAIDS) v2.1
b Based on a ULN of 1.2 mg/dL.
c Based on a ULN of 47 U/L.
d Based on a ULN of 38 U/L.
RECOMMENDED DOSE
The recommended dosage of EBANGA™ for adult and pediatric patients is 50 mg/kg administered as a single IV infusion over 60 minutes. EBANGA™ must be reconstituted with Sterile Water for Injection, USP then further diluted in 0.9% Sodium Chloride Injection, USP or 5% dextrose Injection, USP prior to IV infusion.
Important Safety Information
WARNINGS AND PRECAUTIONS
Hypersensitivity Reactions Including Infusion-Associated Events: Hypersensitivity reactions including infusion-associated events have been reported with EBANGA™. These may include acute, life-threatening reactions during and after the infusion. Monitor all patients for signs and symptoms including, but not limited to, hypotension, chills and elevation of fever, during and following EBANGA™ infusion. In the case of severe or life-threatening hypersensitivity reactions, discontinue the administration of EBANGA™ immediately and administer appropriate emergency care.
Infusion could not be completed in 1% of subjects who received EBANGA™ due to infusion-associated adverse events. The rate of infusion of EBANGA™ may be slowed or interrupted if the patient develops any signs of infusion-associated events or other adverse events.
ADVERSE REACTIONS:
The most frequently reported pre-specified infusion-related adverse events (≥5%) that occurred during EBANGA™ infusion were pyrexia (fever), tachycardia, diarrhea, vomiting, hypotension, tachypnea, and chills.
The following pre-specified symptoms, which were assessed on a daily basis during admission while admitted to the treatment unit, were reported in ≥40% of participants who received EBANGA: diarrhea, pyrexia, abdominal pain, and vomiting. Evaluation of these symptoms may have been confounded by the underlying Orthoebolavirus zairense infection.
DRUG INTERACTIONS:
No vaccine-therapeutic interaction studies have been performed in human subjects using EBANGA™. However, because of the potential for EBANGA™ to inhibit replication of a live vaccine virus indicated for prevention of Orthoebolavirus zairense infection and possibly reduce the efficacy of the vaccine, avoid the concurrent administration of a live vaccine during treatment with EBANGA™. The interval between administration of EBANGA™ therapy and live vaccination should be in accordance with current vaccination guidelines.* The efficacy of EBANGA™ among subjects who reported receipt of a recombinant live vaccine prior to their enrollment in the trial was similar to subjects who did not report receiving a vaccine prior to enrollment.
Use in Specific Populations
Lactation: Patients infected with Orthoebolavirus zairense should be instructed not to breastfeed due to the potential for Orthoebolavirus zairense transmission.
To report suspected side effects or adverse reactions, contact Emergent BioSolutions at: 1-800-768-2304. If you are based in the United States, you can also contact FDA directly at: 1-800-FDA-1088 or www.fda.gov/medwatch.
For more information, please see the full Prescribing Information for EBANGA™.
*Advisory Committee for Immunization Practices (ACIP) Ebola Vaccine Recommendations | CDC